External and internal load in the context of dose and response
Update: Jan 16th 2026
Physical interventions are used to increase physical (sports) performance and considered as effective low-cost strategies in the fields of healthcare, disease or injury prevention, and medical treatment. In general, a considerable amount of evidence buttress the application of physical interventions in various fields as it has been demonstrated to contribute to the maintenance and recovery of physical performance, cognitive function, and overall state of health. To implement physical interventions effectively, it is essential to provide an appropriate exercise and training prescription. Exercise and training prescription are key for “dose” specification and for the individualization (personalizing) of physical exercise and training, precisely adjusted and controlled like medication. Since the physiological response to physical interventions is demonstrably individual and dependent on many influencing factors, individualization is an emerging approach aiming to maximize the efficiency of an intervention by accounting for the interindividual heterogeneity. The present overview aims to distinguish and to redefine between the terms dose and response in order to improve the understanding of practitioners, the methodology of study protocols, and to relate future findings to the actual biological (interindividual) variability of acute and chronic responses. In addition, different approaches to prescribe physical interventions with its advantages and disadvantages are discussed.The basis for this overview is provided by our linked perspective articles from 2020. Finally, we will place relevant perspective and review articles from the international research literature into the context of the topic in order to complete the overview.


It’s not just what you do, it’s how your body responds
There is growing evidence that regular physical activity and/or physical exercise (as planned, structured, and purposive forms of physical activity) lead to positive effects on physical performance and health in various physiological subsystems (e.g., metabolic, cardiovascular, musculoskeletal, or central nervous system) and the organism as a whole, which emphasizes its use in different fields of application. Hence, “physical interventions“, which serve as an umbrella term that covers “physical exercise” (as an acute single bout of physical exercise) and “physical training” (as regularly conducted and multiple bouts of physical exercise), are used and have been proven to be an effective low-cost strategy to recover, maintain or increase physical (sports) performance or the overall health status of an individual in different fields of application (e.g., healthcare, disease and injury prevention, medical treatment). To implement physical interventions effectively in physical (sports) performance enhancement, disease prevention, and medical treatments, it is essential to provide an appropriate exercise and training prescription. Such a prescription should consider the fundamental principles of exercise and training prescription (e.g., regularity, specificity, overload, and progression) and should fully specify external load variables (such as exercise and training variables) and internal load variables (see figure below). Furthermore, exercise prescription is key for “dose” or “dosage” (regularly provided dose over a specific period of time) specification and for individualization (personalizing) of physical exercise and training, precisely adjusted and controlled like medication. In the following, this overview is using dose as an umbrella term covering dose and dosage and will be defined in the later sections.
Below an overview of relevant factors for individual physical exercise and training prescription based on specific objectives and the respective context in the varying fields of application can be found, as well as principles for the programming and monitoring of physical exercise and training. The dose–outcome relationship, which will be defined later in the text, depends on a multitude of factors, such as factors of external and internal load and influencing factors (HR: heart rate, HRV: heart rate variability, VO2: oxygen uptake, RER: respiratory exchange ratio, CK: creatine kinase, CNS: central nervous system, RPE: rating of perceived exertion, DOMS: rating of delayed onset muscle soreness, PAP: post-activation potentiation, FOR: functional overreaching, NFOR: non-functional overreaching, OT: overtraining):

Here, intensity often referred to as main driver of acute and chroncic responses, can be understood as a composite metric that cannot be captured by a single variable of either external or internal load. For example, on the external load side, intensity (e.g., controlled via wattage in cycling) is strongly influenced by factors such as the duration of an exercise bout or movement frequency (here, as cadence). Environmental conditions (e.g., temperature, humidity, or natural altitude) also affect intensity. On the internal load side, it is likewise unlikely that any single measurement variable can adequately represent intensity for the organism as a whole for purposes of control or feedback.
An example from our camping vacation illustrates an analogy. Our toaster was set to intensity level 3 out of 6, and in the picture you can see the first toast (left) and the third toast (right). The duration of exposure to the selected intensity level was the same. However, the operating time of the heating coil increased, meaning that the respective starting temperature also influenced the degree of browning of the toast. Indirectly, therefore, the uninterrupted operating duration of the toaster played a role. The browning of the toast can be seen here as analogous to internal load - roastet:
Since the physiological response to physical interventions is demonstrably individual and dependent on many influencing factors, individualization is an emerging approach which aims to maximize the efficiency of an intervention by accounting for the interindividual heterogeneity in athletes, healthy populations and patients. Therefore, it is necessary to evaluate the actual interindividual differences in acute psychophysiological response(s) to the same acute physical exercise and/or adaptations to the same physical training. To take interindividual heterogeneity into account, a discussion about the classification of “responder”, “non-responder”, “adverse responder”, or “individuals who did not respond” has been emerged, but a generally accepted agreement on an appropriate classification approach has yet not been reached. However, the extent of the individual physiological response to physical interventions (sensitivity to respond to the given stimuli) need to be referenced relative to a specific outcome in the variable of interest according to the initial objective. The interindividual responsiveness to physical interventions and, in turn, the interindividual heterogeneity in outcomes are caused by several moderators, including non-modifiable factors (e.g., sex or genotype) and modifiable factors (e.g., nutrition, social or cognitive activities, exercise prescription). Moreover, it is assumed that low-sensitive responsiveness can be best counteracted by modifying the dose of the physical exercise and/or physical training. The latter suggests that the dose of physical interventions per se contributes significantly to the observed interindividual heterogeneity of specific outcomes. In a recent systematic review and meta-analysis, Greenham et al. (2018) identified biomarkers of physiological responses associated with altered exercise performance following intensified physical training. The majority of the identified biomarkers demonstrated inconsistent findings, due in part to large interindividual response heterogeneity. The authors recommending that future research should strengthens the focus on individual responses rather than group responses and factors that contribute to the interindividual variability in response.
Examples of possible proxies for psychophysiological responses and internal load for exercise prescription and monitoring purposes – rating of perceived exertion serves as representative for the assessment of psychometric scales as subjective indicators of internal load:

Redefining dose and response for individualized physical exercise and training prescription
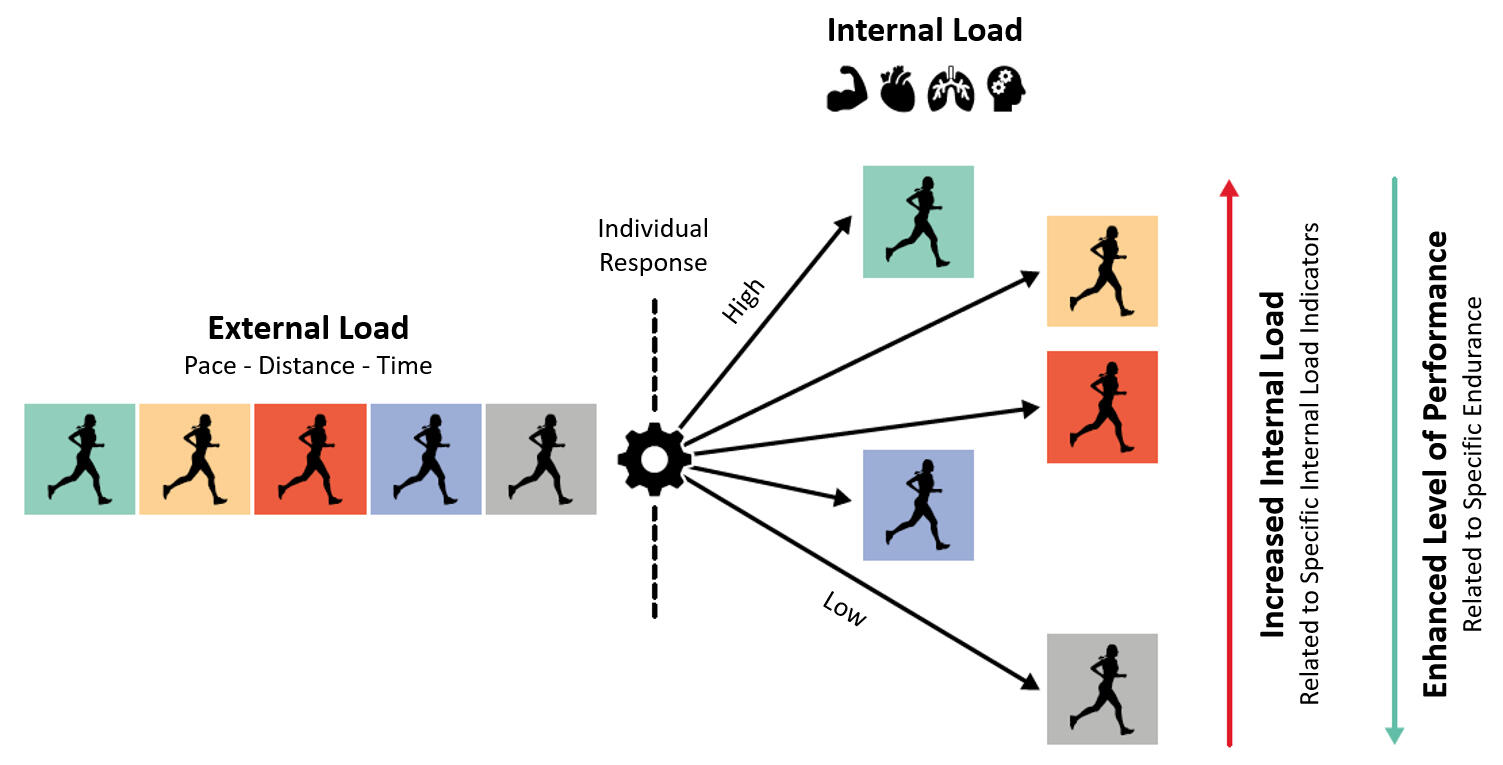
An adequate physical exercise and training prescription is a key element in science and practice to characterize the dose of physical interventions. While the term dose–response (relationship) is very frequently used in the media as well as in scientific literature, it is usually not defined what is meant by “dose” and which “response” is being referred to.In order to define the dose of a physical intervention, three key components should be considered: (1) external load (defined as the work completed by the individual independent of internal characteristics), (2) influencing factors (all factors that can strengthen or disturb the stimuli of a single bout of exercise and/or training), and (3) internal load (defined as the individual and acute physiological, psychological, motor, and biomechanical responses to the external load and the influencing factors during and/or after the cessation of a single bout of physical exercise). The figure above gives an overview of the multitude of factors in the subcategories, without claiming to be complete. In this regard, parameters of external load (e.g., running with a speed of 10km/h or swimming with a pace of 65 s per 100 m) or parameters of internal load (e.g., running with 70% of maximum heart rate) can be used to prescribe and control exercise intensity (or at least an important part of it). Here, the internal load has a key role in physical exercise and training prescription as it represents the crucial impetus for acute and/or chronic changes. Hence, we propose that dose can be operationalized and monitored using a specific indicator (or set of specific indicators) of internal load as proxy. In this regard, it is mandatory to distinguish with respect to the number of exercise sessions between a single bout of physical exercise (i.e., one session leads to an internal load) and repeated bouts of physical exercise defined as training (i.e., several and consecutive sessions during a defined period lead to repeated bouts of internal loads). Whereas a single bout of physical exercise leads to distinct acute responses shown by a transient reaction of the organism (beneficial, maintaining, or detrimental depending on the stimuli), repeated bouts of physical exercise ultimately converge into distinct chronic responses or adaptations (beneficial, maintaining, or detrimental depending on the stimuli).Below a schematic illustration of individual responses related to the same external load situation can be found with an example of running. An increased internal load (e.g., heart rate response) allows the assumption that there is a lower specific level of capacity and endurance performance in terms of running:
Consider a simple analogy with two people run on treadmills side-by-side at the exact same speed. They are exposed to an identical external load. However, one might be a seasoned marathoner whose heart rate is a steady 130 bpm, while the other is a beginner who is completely exhausted with a heart rate of 180 bpm. They are experiencing vastly different internal loads. This distinction is the foundational reason why one-size-fits-all plans fail—they only control the work, not the physiological stimulus it creates.With regard to our definition of dose, and given that internal load as acute response is a part of dose, the term “response” in the frequently used phrase “dose-response (relationship)” should be specified as “chronic response” (effect on a specific outcome parameter, e.g., mitochondrial volume and density) in the meaning of adaptation as a potential result of several and consecutive sessions of physical exercise. To be even more precise and to broaden the understanding of the dose-response relationship, we recommend redefining the phrase “dose-response” as “dose-outcome”, which specifies the link to an acute outcome parameter (in regard to a single bout of physical exercise) or a chronic outcome parameter (in regard to repeated bouts of physical exercise defined as training) according to the respective objective(s). In this context, dose could be seen as an independent variable or a set of independent variables which we assume to be involved in biological processes in general and in a complex response matrix and signal transduction, specifically leading to a distinct “outcome” (dependent variable). However, according to the definitions, internal load as proxy of the dose could be controlled by modifying the external load in consideration of exercise and training principles (e.g., periodization for the planned systematic and structural variation of a training program over time with an adequate relationship of load and recovery periods) and influencing factors such as the actual state of the psychophysiological capacity level (including level of performance).Given that an adequate exercise and/or training prescription is pivotal to administering an effective dose, this ongoing debate might produce major sources of difficulty in implementing physical exercise as medicine. Having said this, such a debate also entails great potential to serve as a promising starting point for fostering progress in both research and practical settings. To contribute to this debate, we will explain different approaches to prescribing and tailoring physical interventions from this perspective by highlighting their potential impact on interindividual heterogeneity regarding health- and perforamnce-related outcomes.
Four different roads to prescribing physical interventions
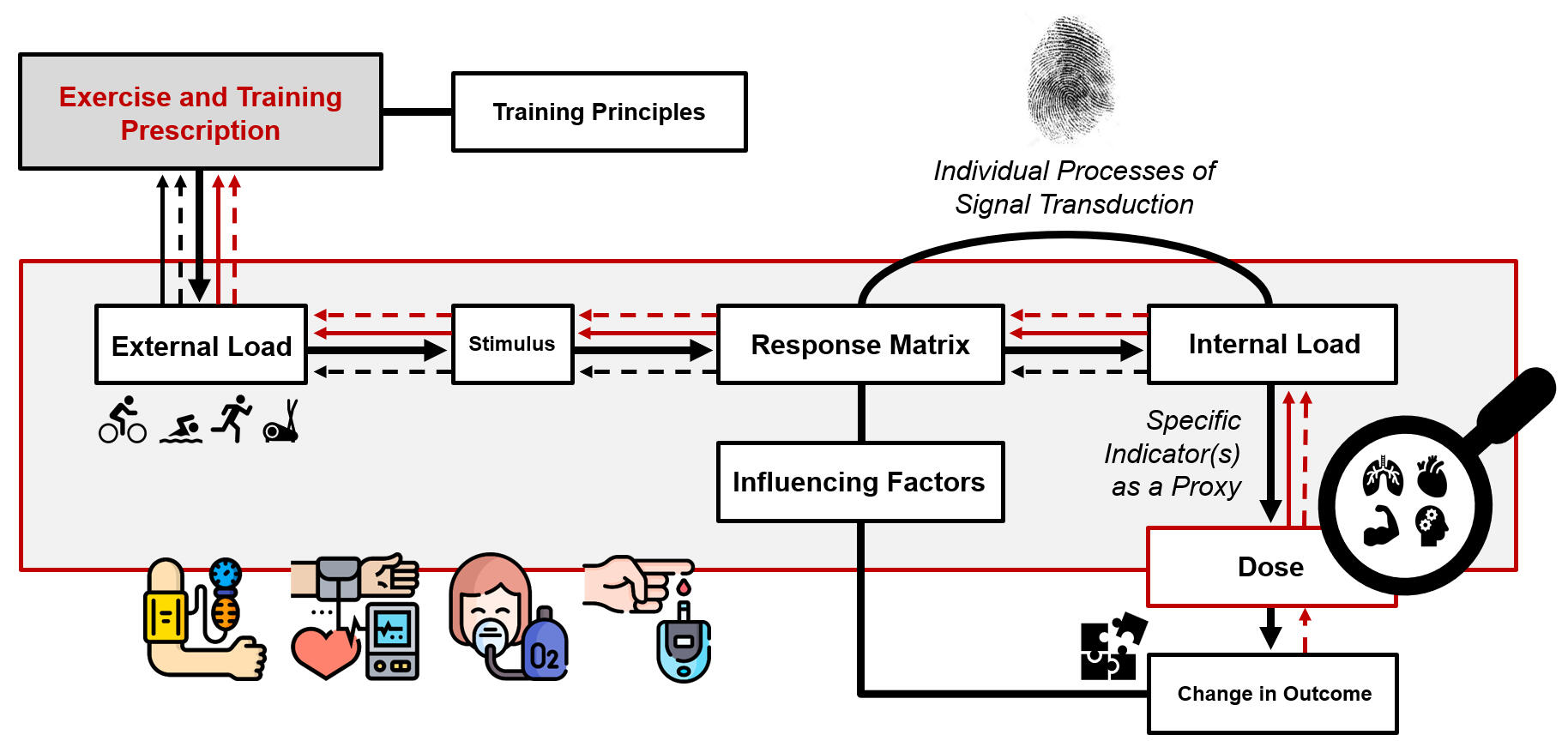
In this section, an overview of approaches that can be used to prescribe physical interventions is given. Furthermore, it is shown how different approaches to exercise and/or training prescription can potentially influence the dose and outcome. In this regard, it is postulated that there are four approaches to prescribe physical interventions: approach (1) is based on the parameter(s) of external load to ensure a comparable external load across different individuals; approach (2) is based on indicator(s) of internal load to ensure a comparable internal load across different individuals; approach (3) aims to achieve a comparable dose across different individuals; and approach (4) aims to achieve a comparable outcome (or a comparable change in an outcome) across different individuals (see figure below). In this regard, we define outcome (dependent variable) as a specific parameter of interest that is a function of the dose (independent variable). It is, however, worth noting that a clear assignment of a distinct variable, either to our concept of dose or to our concept of outcome, is highly context-specific. The application of those two prospective approaches (especially approach (3), based on a comparable dose) could be promising for gaining further insights into the effects of exercise and/or training prescription on biological processes and specific outcomes. Below, however, all four approaches of exercise and/or training prescription are discussed in more detail.Schematic illustration of four approaches to prescribe physical interventions. Approaches are based on (1) comparable external load (solid black line), (2) comparable internal load (dashed black line), (3) comparable dose (solid red line), or (4) comparable outcome (dashed red line). The prescription of physical interventions is based on different exercise variables, training variables, and training principles inducing a specific exercise stimulus. In the so-called response matrix, the exercise stimulus interacts with the unique characteristics of the individual which leads to a measurable psychophysiological response (i.e., internal load). In short-term, a specific internal load can cause acute changes in distinct outcome parameters whereas the repetitive and long-term occurrence of an internal load can drive chronic changes in distinct outcome parameters (e.g., adaptations). Such chronic changes influence modifiable individual factors (i.e., capacity level) which, in turn, alter the biological processes in the response matrix:
(1) Comparable external load
A prescription using a comparable external load ensures that every participant exercises with the same parameters of external load (e.g., exercise prescription with each individual cycle at 60% of their peak power output for 20 min, for example, as previously determined by a performance test). This approach to exercise and/or training prescription is relatively easy to apply, but, on the other hand, it can cause considerable interindividual heterogeneity with respect to the internal load, the dose, and the outcome due to interindividual differences in performance capacities in various biological subsystems. However, the exercise and/or training prescription based on a comparable external load can be favorable when the other approaches are hardly practicable and/or are not sufficiently reliable (e.g., in high-intensity interval training with relative short intervals, sprint interval training, or repeated sprint training).
(2) Comparable internal load
By using an exercise and/or training prescription relying on a comparable internal load, it is ensured that an indicator of internal load is comparable across different individuals (e.g., an exercise prescription ensuring that each individual runs within 60% of maximum heart rate for 20 min, as previously determined by a performance test). This approach is more favorable than approach (1), as markers of internal load take individual characteristics and environmental factors into account and reflect acute biological response(s), which are the crucial impetus for acute and chronic biological changes. However, approach (2) has also limitations: (a) we often do not know which indicator or set of indicators of internal load is/are the crucial impetus for triggering biological processes leading to specific and intended changes, and (b) a prescription based on a specific indicator of internal load (e.g., maximum oxygen uptake or heart rate) induces a considerable heterogeneity in other indicators of internal load (e.g., level of peripheral blood lactate concentration). Therefore, this approach is likely to cause a relatively large interindividual heterogeneity with respect to the dose and the outcome – especially when considering only percentage relations to maximal ankers of performance testing compared to relationships to submaximal physiological thresholds.
(3) Comparable dose
A prescription that aims to achieve a comparable dose attempts to refine an approach based on a comparable internal load (see previous paragraph (2) comparable internal load). In this regard, one or multiple specific indicators of internal load serve as proxy of the dose and are comparable across different individuals. Here, it is a necessary to emphasize (a) that these specific indicator(s) of internal load serving as a proxy of the dose are assumed to be or are known to be (causally) involved in biological processes leading to the change in the intended outcome and (b) that a specific internal load will be achieved by a careful and individual adjustment of external load (while taking influencing factors into account). Based on this approach, it has been hypothesized that, for instance, the peripheral blood lactate concentration could be a promising proxy for prescribing physical interventions in exercise-cognition research, since there seems to be a neurophysiological relationship between the amount of the peripheral blood lactate concentration and neurocognitive changes. The strong rationale for using specific biological responses in exercise and/or training prescription to achieve specific, but comparable stimuli across different individuals is a clear advantage and supports the use of this approach. In some settings (e.g., endurance training), similar approaches are already used, but in other settings (e.g., neuroscience), their practical implications should be more frequently considered (e.g., influence of a comparable dose on the interindividual heterogeneity of a specific neurocognitive outcome). The application of a dose-related approach will lead to new insights explaining the relationships between exercise and/or training prescription, biological processes, and outcomes. Such new insights could, at least in part, pave the way for an approach to prescribing physical interventions that leads to a relatively comparable outcome across different individuals (see the next approach (4) comparable outcome) and might also contribute to a refinement of the current concept of dose in physical interventions.
(4) Comparable outcome
A prescription aiming to achieve a comparable outcome (or a comparable change in an outcome) across different individuals would be the most desirable approach to exercise and/or training prescription, as it maximizes the benefit for the single individual according tot he initial aim(s). This approach is based on a highly tailored exercise and/or training prescription that requires a flexible adjustment of the exercise and training variables to achieve the intended outcome. Consequently, this approach leads to a relatively large interindividual heterogeneity in parameters of external load and various indicators of internal load. In this case, the impact on the dose is currently relatively unclear. However, it should be considered that a comparable outcome (or a comparable change in an outcome) cannot be achieved in every circumstance, as individual capacities of biological subsystems (e.g., musculature) are limited (i.e., not every individual will be able to run 100 m in less than 10 s). Although it might be difficult to achieve a comparable outcome (or a comparable change in an outcome) across different individuals under some circumstances, this does not challenge the basic idea of this approach which states that a rigorous individualization of the exercise and/or training prescription (e.g., due to a flexible and individual adjustment of the external and internal load) is necessary to obtain a specific and intended outcome. With respect to health-related outcomes, an interindividual comparable outcome (or a comparable change in an outcome) is, in general, possible to obtain, as an individual optimum in a specific outcome is situated within a “normal” physiological state that can be aimed for (e.g., resting blood pressure around 120/80 mmHg). The same could be applied for a performance-related outcome with the aim to optimize or maximize this metric (e.g., maximum oxygen consumption). In this regard, it is worth noting that approaches (1), (2), and (3) are outcome-oriented as well. In particular, the established approaches (1) and (2) are based on the prescription of specific exercise and training variables of which we know (e.g., based on findings from a meta-analysis) that they lead, in general, to a certain change in an outcome parameter. However, under most circumstances, when applying approaches (1), (2), and (3), one would not need to consider interindividual differences in the capacities of all biological subsystems in the exercise and/or training prescription. As a result, these approaches do not necessarily induce comparable outcomes across different individuals, although further research is necessary to support this assumption empirically with respect to approach (3). To come closer to a highly tailored exercise and/or training prescription as intended in approach (4), two strategies for research in this field can be applied: (a) investigating how a comparable dose across different individuals would influence a specific outcome (see approach (3) comparable dose) and (b) investigating how achieving a comparable outcome across different individuals would influence dose. To realize strategy (b), N-of-1 studies could be a promising option. An N-of-1 study is a randomized controlled trial that is conducted in a single individual and is performed with a within-subject design with multiple crossovers. In such an N-of-1 trial, the exercise and/or training prescription for the single individual needs to be systematically adjusted to change the dose and, in turn, to elucidate its effect on a specific outcome (e.g., this approach is often used in high-performance sports to determine an optimally tailored exercise and/or training prescription for an individual athlete). To draw conclusions regarding comparability and interindividual heterogeneity, such N-of-1 studies, of course, need to be conducted with several independent participants. Probably such a systematic variation of the exercise and/or training prescription in N-of-1 studies help us to better understand the underlying biological processes that lead to a specific outcome and to identify the most appropriate prescription of phsical interventions (e.g., best indicator(s) of internal load) to achieve the optimal dose and to maximize, in turn, the benefits for the individual. These theoretical assumptions, however, need to be proven empirically by performing well-designed N-of-1 studies.In addition, the following important points are applicable to all of the above-mentioned approaches to exercise and/or training prescription and should be considered when designing and analyzing physical interventions. Based on their temporal characteristics, outcome should, additionally, be classified into (a) acute change in an outcome in response to a single and acute bout of physical exercise, and (b) chronic change in an outcome in response to several exercise sessions over a distinct time period. In this context, the stimulus of acute physical exercise triggers an acute and transient physiological, psychological, motor, and biomechanical response during (e.g., transient increase of heart rate) and/or after the cessation of the single bout of physical exercise (e.g., transient increase of endocrine hormones), which leads to an acute and transient change in an outcome (e.g., change in blood pressure such as post-exercise hypotension). Regularly performed physical exercise over a distinct time period causes chronic response(s)/organismic adaptation(s) (e.g., basal change in endocrine hormone level or change in arterial stiffness level) which, in turn, contribute substantially to a permanent change in a distinct outcome parameter (e.g., decrease in resting systolic/diastolic blood pressure). Furthermore, it is important to mention that wearable devices and smartphone applications offer great potential to tailor, prescribe, and monitor physical interventions although a stricter scientific evaluation is often needed with regard to commercially available devices/applications for such monitoring purposes. Notably, it has been shown that smartphone apps can positively influence exercise adherence (e.g., by providing feedback and motivation), which is an important factor determining the effectiveness of a physical intervention. However, to fully harness the great potential of wearable devices and smartphone applications in exercise and/or training prescription, further research in this direction is urgently needed.
Practical implications and areas for future research
Valid indicators that represent the most appropriate proxies of dose for prescribing physical interventions are highly specific and more research is needed to identify them (with regard to the context and/or specific acute or chronic responses). In this regard, current concepts discuss promising internal load parameters (e.g., brain-derived parameters, hormones) to prescribe physical exercise, in addition to traditional measures like heart rate, blood lactate concentration, or rating of perceived exertion. Nevertheless, there is a good, at least theoretical, rationale in support of the individualization of exercise and training prescription by providing a distinct (comparable and standardizable) dose across individuals to elicit the desired psychophysiological responses, which would in turn allow for a better comparison of outcomes across different individuals. Therefore, existing recommendations endorse the adequate prescription of single exercise sessions and/or training with the specification of parameters of external load and markers of internal load in science and practice.The approach used for exercise and/or training prescription has a considerable impact on comparability across different individuals and the interindividual heterogeneity of parameter(s) of external load, indicator(s) of internal load, dose, and outcome. These fundamental differences between approaches to exercise and/or training prescription should be considered when designing physical interventions or when analyzing the effects of physical interventions. However, the most suitable and effective parameters for a prescription are, so far, relatively unknown, which, on the one hand, limits the conclusions that can be drawn with certainty, but, on the other hand, also highlights the need for further research in this direction. From a practical and theoretical point of view, it can be unreservedly recommended (a) that, in general, specific markers of internal load should be used to prescribe and monitor physical interventions, (b) that the adaptation of internal load requires the careful and individual adjustment of external load (while taking influencing factors into account), (c) that both parameter(s) of external load and indicator(s) of internal load should be reported in detail to enhance comparability and reproducibility of physical interventions, and (d) that the most suitable exercise and/or training prescription is probably achieved by considering empirical evidence and performing interdisciplinary teamwork (e.g., integrating the perspectives of patients and the expertise of medical experts, sport scientists, and practitioners). However, the continuous improvement of the prescription of physical interventions warrants further, arguably more critical investigation. In this regard, it is necessary to conduct further well-designed cross-sectional studies (e.g., to explore possible relationships between indicator(s) of internal load reflecting biological processes and specific outcome(s)) and longitudinal studies (e.g., to prove causality and effectiveness of such an approach) to broaden our understanding of the relationships between the exercise and/or training prescription, the underlying biological processes, and the outcome. Accordingly, we strongly advocate investigating whether physical interventions with a comparable dose between different individuals influences the interindividual heterogeneity in distinct health-related and/or performance outcomes.In the following section, additional approaches are presented that point in a similar conceptual direction. However, these approaches partly rely on differing definitions and uses of key terms, which are not always applied consistently across the literature.
Comparable conceptual directions in the literature
The framework proposed by Vanrenterghem et al. (2017) introduces a critical distinction between physiological and biomechanical load-adaptation pathways to improve training precision and injury prevention, here especially with the focus on teams sports. While physiological monitoring focuses on metabolic and cardiovascular energy consumption, the biomechanical pathway centers on the mechanical stresses placed on musculoskeletal tissues, including tendons, bones, and cartilage.

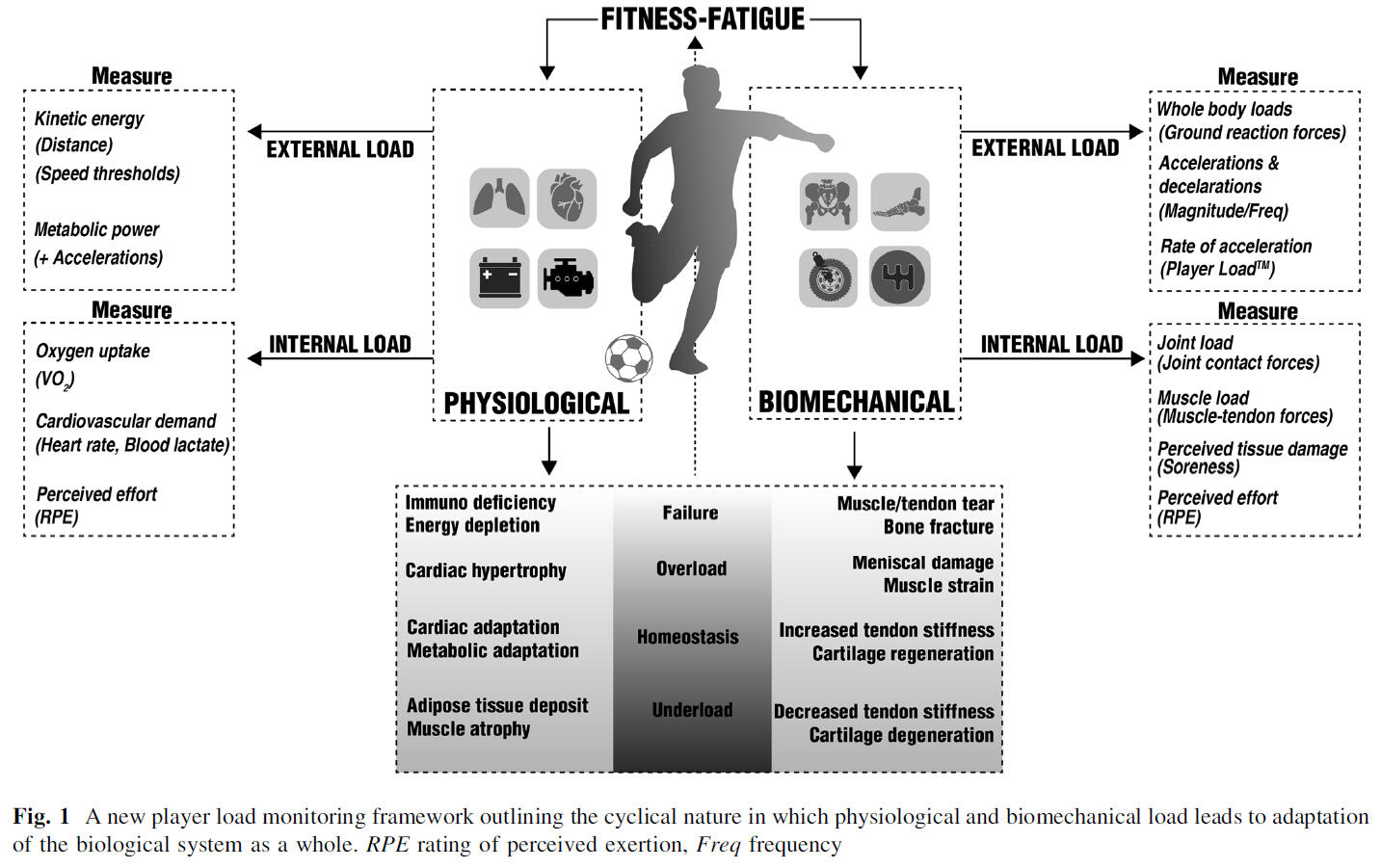
Key biomechanical aspects of this framework include:
Load differentiation: External biomechanical load is characterized by the forces generated against the environment (e.g., ground reaction forces), which are often estimated using accelerometry-based measures. Internal biomechanical load refers to the resulting tissue-specific stresses, such as joint contact forces and muscle-tendon forces.
Adaptation and response rates: Unlike physiological systems (e.g., energy depletion/replenishment), biomechanical tissues adapt through changes in tissue properties, such as increased tendon stiffness or cartilage regeneration. A central tenet of the framework is that biomechanical adaptations often have a slower response rate than physiological ones.
Risk of tissue failure: Because of these different timescales, an athlete may appear physiologically recovered while their musculoskeletal system remains in a state of "critical weakness". If the next high biomechanical load is delivered before the tissue has adapted, it can lead to gradual degeneration and eventual tissue failure or injury.
Practical application: Practitioners can use this framework to independently manipulate loads. For instance, aqua jogging, anti-gravity treadmills, or running on sand can be used to provide a high physiological stimulus while significantly reducing the biomechanical impact on the body.
The articles by Foster et al. (2017) and Impellizzeri et al. (2019) provide a critical update to the theoretical framework of the training process, focusing on the distinction between the work performed and the body’s reaction to it with a further detailed look on the specification of training load. The authors posit that exercise serves as a stressor that induces various psychophysiological responses, and it is this internal response—rather than the exercise task itself—that provides the actual stimulus for biological adaptation. By separating the training process into measurable constructs, the framework allows for more precise control over the stress applied to an athlete. The authors argue that while technology has made the measurement of external load (e.g., distance, speed, power) increasingly accessible, practitioners should prioritize the internal load. This is because individual characteristics such as genetics, training status, and health mean that the same external task can result in vastly different internal strains for different athletes. Ultimately, these frameworks serves as a guide for integrating these two load types to optimize training outcomes and prevent maladaptations like overtraining.

Drawing from these sources, the "dose" of physical training is formally defined and operationalized through the concept of training load:
As an input variable: Training load is defined as the input variable that is systematically manipulated to elicit a desired training response.
A two-Component construct: The dose consists of the interaction between external training load (the physical work prescribed or completed, such as distance or kilograms lifted) and internal training load (the actual psychophysiological response initiated by the body to cope with the external requirements).
Quantitative formula: As noted by Foster et al. (2017), the dose is often expressed quantitatively as the product of frequency, intensity, and time. This is commonly captured through indices like training impulse calculations (TRIMP) or session rating of perceived exertion (sRPE), which serve as mathematical surrogates for the total biological stimulus experienced by the athlete.
The effective stimulus: Crucially, the sources emphasize that the internal load represents the "dose" in its most biologically relevant form, as it is this internal demands that directly leads to the transient acute responses and long-term chronic adaptations required for performance.


Although the authors present the distinction between internal and external training load as a conceptual framework introduced in 2003, it is important to note that this paradigm has a much longer history in German research. As early as the 1970s and 1980s, German occupational science systematically operated with the concepts of external load ("Belastung") and internal load ("Beanspruchung"), supported by well-established theoretical models related to work place environments. In the early 1990s, this framework was explicitly transferred to endurance training by the research groups around Georg Neumann and Kuno Hottenrott, who published extensively on the relationship between external (training) load and internal physiological responses and influencing factors, accordingly. However, these contributions were almost exclusively disseminated in German-language publications and therefore remained largely unnoticed in the international literature.
In an overview by Jeffries et al. (2021) a comprehensive revised conceptual framework for physical training was presenetd, designed to provide a solid theoretical foundation for both scientific research and practical athlete monitoring. The authors highlight that the sports science field often suffers from a lack of conceptual clarity, particularly regarding subjective measures, which can lead to biased interpretations and poor methodological foundations. To address this, the researchers synthesized existing literature and integrated established mathematical models—such as the Banister Impulse-Response model and the PerPot metamodel—to create a unified structure. The model resembles the above-mentioned model developed by our research group and incorporates individual and contextual factors, and both acute and chronic positive as well as negative effects.

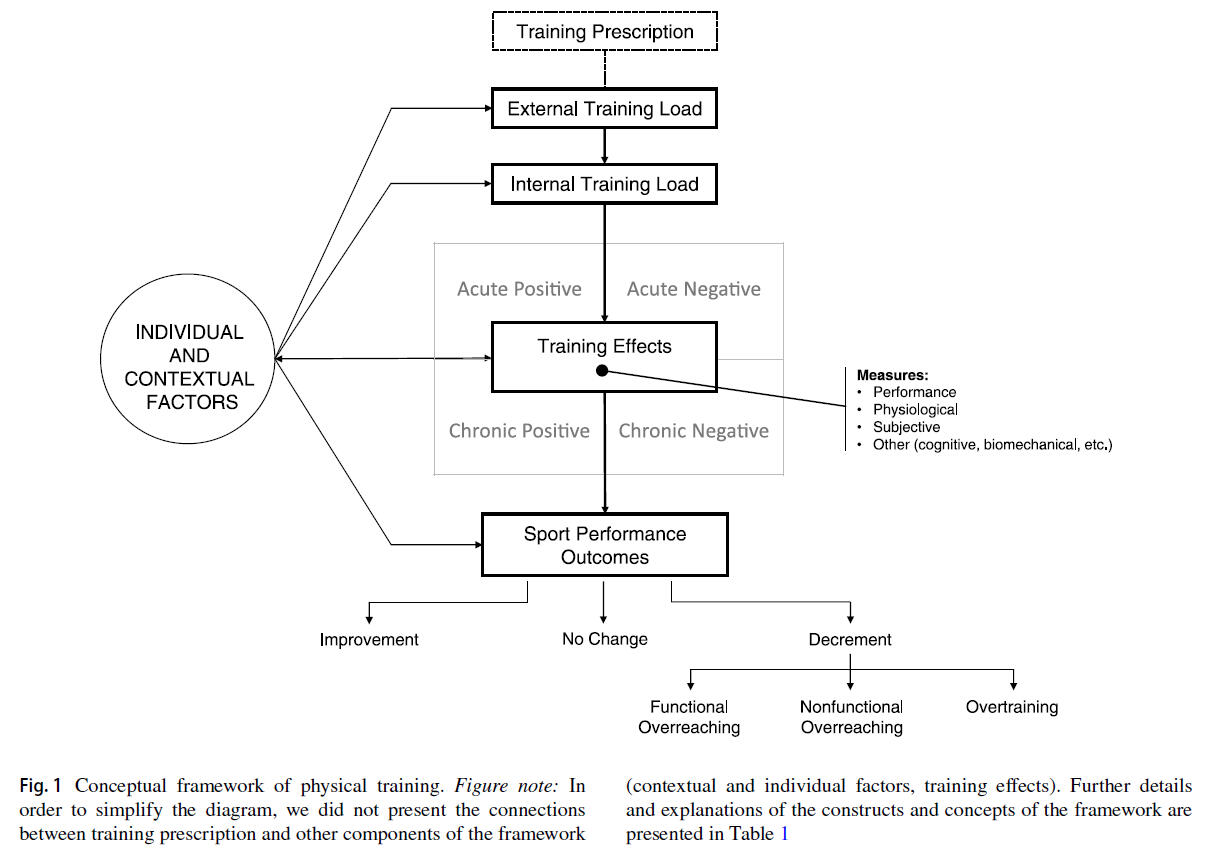
The proposed framework is built around four central expanded constructs; (1) a measurable component resulting from the combination of four possible responses – acute vs. chronic and positive vs. negative effects, (2) an explanation of how physiological, performance-based, and subjective data serve as indicators of these effects, (3) a continuum of results ranging from performance improvement to non-functional overreaching and overtraining, and (4) a network of modifiable and non-modifiable individual variables and contextual factors (e.g., genetics, nutrition, environment) that maintain bidirectional relationships with the training process and its effects.
Ultimately, this framework serves as an operational guide for validating measurement instruments and interpreting data to optimize individual training responses. The concept of "dose" is formally defined and operationalized through the higher-order construct of training load. The framework establishes several key characteristics to define this dose:
Actual experience vs. plan: The dose is explicitly defined as the amount of physical training that is actually done and experienced by the athlete. The sources make a clear distinction between the "training prescription" (the intended plan) and the "training load" (the actual dose received).
The external load component: This represents "what the athlete does". It is the objective, observable physical work performed during a session, such as distance covered, speed, power output, or the amount of weight lifted.
The internal load component: This refers to the internal psychophysiological responses experienced by the athlete during the exercise. These responses—such as heart rate, blood lactate levels, or the rating of perceived exertion—represent the biological stimulus.
Causal role of the dose: Within this framework, the external load interacts with individual and contextual factors to determine the internal load. This internal load is considered the crucial biological dose that acts as the stimulus to initiate subsequent acute or chronic training effects.
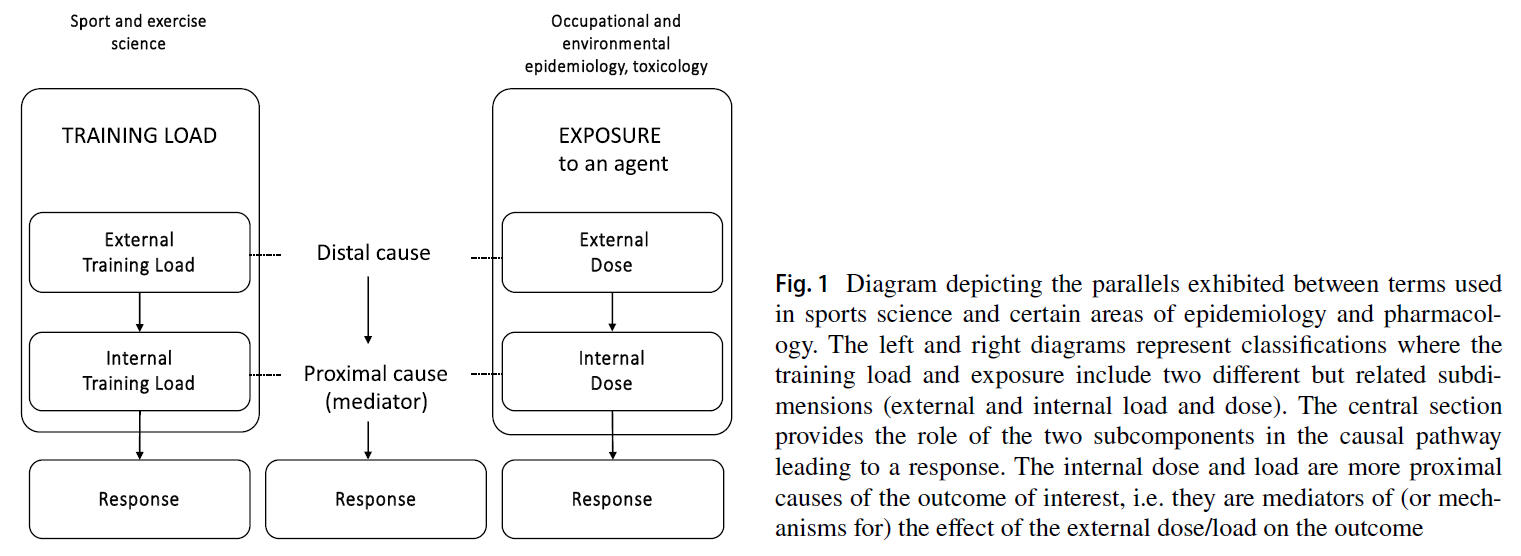
Finally, the article by Impellizzeri et al. (2023) explores how the concepts of physical training load can be aligned with established classifications in epidemiology, pharmacology, and occupational medicine. The authors describe training load as a multidimensional construct consisting of two causally related subdimensions: external and internal load. By applying a causal inference perspective, the framework illustrates that training functions as an "exposure" where the internal load acts as a mediator for the effects of the external load on performance or health outcomes. The article emphasizes that for any measure of training load to be practically useful for optimizing the training process, it must be reflective of the specific mediating mechanisms (mechanistic stimuli) that drive the desired biological adaptation. Furthermore, the authors argue that while technology allows for the collection of vast amounts of data, a measure is only valid in a causal context if it can be linked to a plausible mediator of the relevant response.

In this article, the authors explicitly reconcile the terminology of sports science with other scientific disciplines to define "dose" as follows:
Equivalent to load: The term "load" is considered the conceptual equivalent of "dose", referring to the amount of a specific factor or agent. While the terms are often used interchangeably, "load" is preferred in sports science because it also conveys the idea of demands and challenges imposed on the organism.
Interaction with the organism: Drawing on epidemiological definitions, dose is specifically defined as "the amount of a factor [or agent] that enters or interacts with the organism". This represents the actual stimulus that triggers biological adaptations.
External vs. internal dose: The framework differentiates between two types of dose – (1) external dose (external load) – defined as the amount of training (activities and actions) to which individuals are exposed – it represents "what athletes do", and (2) internal dose (internal load) – defined as the internal psychophysiological stress an individual experiences to cope with the demands of the external load. The internal dose is the proximal cause of the outcome and the mediator that ultimately determines adaptations.
Further ressources
In our overview article, we transfer the proposed concepts of dose and response to practical application for intensity control and monitoring in endurance exercise and training. The full text is published in German language and can be requested via Research Gate:

In our new book "Voll im Takt - Ausdauertraining im Rhythmus des Herzschlags: Herzfrequenz messen, Training individualisieren, Bestleistung erzielen" co-authored with Dr. Alexander Törpel we summarized an overview about the background and practical application of dose and response with a focus on heart rate and heart rate variability monitoring for exercise and training prescription with many practical examples and valuable information about wearable technology. The book is written in German language:

Bibliography
Below you can find a bibliography of reviews and perspective articles related to this topic.
Foster, C., Rodriguez-Marroyo, J. A., & de Koning, J. J. (2017). Monitoring Training Loads: The Past, the Present, and the Future. International Journal of Sports Physiology and Performance, 12(Suppl 2), S22–S28. https://doi.org/10.1123/ijspp.2016-0388
Greenham, G., Buckley, J. D., Garrett, J., Eston, R., & Norton, K. (2018). Biomarkers of Physiological Responses to Periods of Intensified, Non-Resistance-Based Exercise Training in Well-Trained Male Athletes: A Systematic Review and Meta-Analysis. Sports Medicine (Auckland, N.Z.), 48(11), 2517–2548. https://doi.org/10.1007/s40279-018-0969-2
Gronwald, T. & Törpel, A. (2024). Voll im Takt – Ausdauertraining im Rhythmus des Herzschlags: Herzfrequenz messen, Training individualisieren, Bestleistung erzielen. München: Riva Verlag. ISBN: 978-3-7423-2564-8
Gronwald, T., Schaffarczyk, M., Herold, F. & Törpel, A. (2025). Intensitätssteuerung und Monitoring über Dosis und Wirkung im Ausdauertraining – Praktische Perspektiven für Training und Rehabilitation. Sportphysio, 13(4), 175–189. doi: 10.1055/a-2625-2217
Gronwald, T., Törpel, A., Herold, F., & Budde, H. (2020). Perspective of Dose and Response for Individualized Physical Exercise and Training Prescription. Journal of Functional Morphology and Kinesiology, 5(3), 48. https://doi.org/10.3390/jfmk5030048
Herold, F., Törpel, A., Hamacher, D., Budde, H., & Gronwald, T. (2020). A Discussion on Different Approaches for Prescribing Physical Interventions - Four Roads Lead to Rome, but Which One Should We Choose? Journal of Personalized Medicine, 10(3), 55. https://doi.org/10.3390/jpm10030055
Impellizzeri, F. M., Marcora, S. M., & Coutts, A. J. (2019). Internal and External Training Load: 15 Years On. International Journal of Sports Physiology and Performance, 14(2), 270–273. https://doi.org/10.1123/ijspp.2018-0935
Impellizzeri, F. M., Shrier, I., McLaren, S. J., Coutts, A. J., McCall, A., Slattery, K., Jeffries, A. C., & Kalkhoven, J. T. (2023). Understanding Training Load as Exposure and Dose. Sports Medicine (Auckland, N.Z.), 53(9), 1667–1679. https://doi.org/10.1007/s40279-023-01833-0
Jeffries, A. C., Marcora, S. M., Coutts, A. J., Wallace, L., McCall, A., & Impellizzeri, F. M. (2022). Development of a Revised Conceptual Framework of Physical Training for Use in Research and Practice. Sports Medicine (Auckland, N.Z.), 52(4), 709–724. https://doi.org/10.1007/s40279-021-01551-5
Mujika I. (2017). Quantification of Training and Competition Loads in Endurance Sports: Methods and Applications. International journal of sports physiology and performance, 12(Suppl 2), S29–S217. https://doi.org/10.1123/ijspp.2016-0403
Vanrenterghem, J., Nedergaard, N. J., Robinson, M. A., & Drust, B. (2017). Training Load Monitoring in Team Sports: A Novel Framework Separating Physiological and Biomechanical Load-Adaptation Pathways. Sports Medicine (Auckland, N.Z.), 47(11), 2135–2142. https://doi.org/10.1007/s40279-017-0714-2